

Volume 13, Issue 3 (10-2018)
Salmand: Iranian Journal of Ageing 2018, 13(3): 396-404 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seghatoleslami A, Hemmati Afif A, Irandoust K, Taheri M. Effect of Pilates Exercises on Motor Performance and Low Back Pain in Elderly Women With Abdominal Obesity. Salmand: Iranian Journal of Ageing 2018; 13 (3) :396-404
URL: http://salmandj.uswr.ac.ir/article-1-1469-en.html
URL: http://salmandj.uswr.ac.ir/article-1-1469-en.html



1- Department of Physical Education, Faculty of Physical Education, University of Birjand, Birjand, Iran. , aseghatoleslami@yahoo.com
2- Department of Physical Education and Sports Science, Faculty of Social Sciences, Imam Khomeini International University, Qazvin, Iran.
2- Department of Physical Education and Sports Science, Faculty of Social Sciences, Imam Khomeini International University, Qazvin, Iran.
Full-Text [PDF 2058 kb]
(4832 Downloads)
| Abstract (HTML) (10482 Views)



مقدمه
امروزه به دلیل اقتضائاتی که در کشور وجود دارد، نسبت جمعیت افراد سالمند به جوان دچار فزونی شده است. با افزایش سن، با وجود ورزش و فعالیت جسمانی، بافتهای عضلانی تحلیل میروند و بافتهای چربی افزایش مییابند؛ از طرفی تغییرات ترکی بدن میتواند زمینه افت عملکرد جسمانی و کنترل حرکتی را ایجاد کند. کمردرد یا درد ستون فقرات نیز از شایعترین عوارض عضلانیاسکلتی است که در دوره سالمندی بیشتر در افرادی مشاهده میشود که سبک زندگی غیرفعالی دارند [1]. یکی از عواملی که ممکن است باعث درد کمر در دوره سالمندی شود، تغییرات ترکیب بدن اعمّ از افزایش توده چربی بدن به ویژه در ناحیه شکم و تحلیلرفتن عضلات در نواحی مرکزی بدن است.
با افزایش چاقی شکمی، قوسی جبرانی در ناحیه انحنای کمری ایجاد میشود. افزایش وزن بالاتنه نیز به دیسکهای بینمهرهای فشار زیادی میآورد و موجب کمردرد میشود [2]. در اثر افزایش قوس ناحیه کمری مرکز ثقل به سمت جلو جابهجا میشود و سبب تغییرات در نحوه گامبرداشتن، اختلال در کنترل پاسچر، افزایش خطر زمینخوردن و کاهش قابلیت جابهجایی حرکتی میشود [3].
یکی از روشهای ورزشی که در سالهای اخیر متخصصان ورزشی و توانبخشی به آن توجه کردهاند و در حال فراگیرشدن است، ورزش پیلاتس است. جوزف پیلاتس در سال 1880 این ورزش را برای اولینبار ابداع کرد. این ورزش مجموعهای از تمرینات تخصصی است که با هدف افزایش قدرت، استقامت و انعطافپذیری، بدن را تحت تأثیر قرار میدهد و از طرفی در کنار بهبود شرایط جسمانی به بهبود مسائل روانشناختی همچون توجه و تمرکز نیز کمک میکند [4]. کاهش بافت عضله در قسمت میانی بدن ممکن است موجب افزایش قوس کمری شود، این موضوع میتواند در سرعت راهرفتن افتی ایجاد کند. کاهش سرعت راهرفتن چنانچه به مقادیر کمتری از ۱ تا 2/1 متر بر ثانیه برسد، برای سالمندان مشکلاتی را در پی خواهد داشت [5]. با وجود تنوع زیاد شیوههای ورزشدرمانی، هنوز دلایل کافی درباره برتری یک روش بر دیگری وجود ندارد.
کائو و همکاران در سال ۲۰۰۷ طی تحقیقی عنوان کردند فعالیت و تمرینات بدنی منظم و مداوم میتواند بهطور مؤثری خطر افتادن را کاهش دهد و تحرک و ایمنی حرکت در زنان مسن را ارتقا بخشد [6]. همچنین آیرز در سال ۲۰۰۹ نشان داده است میتوان با انجام فعالیتهای جسمانی منظم در طول عمر، افت عملکرد حرکتی این افراد را تا حدودی به تأخیر انداخت [7]. سوزوکی و همکاران در سال ۲۰۰۹ طی تحقیقی نشان دادند تمرین و فعالیت بدنی باعث بهبود در تعادل، انعطافپذیری، قدرت عضلانی و توانایی راهرفتن، در افراد سالمند میشود [8].
با توجه به تحقیقات صورتگرفته، مشخص است درباره ورزش سالمندی تحقیقات متنوعی انجام شده است. این موضوع ضرورتی را ایجاد میکند تا در دوره قبلی سالمندی، تمهیداتی صورت پذیرد تا کیفیت زندگی در سالمندی به بهترین شکل تأمین شود. بنابراین، مطالعه حاضر با هدف تأثیر یک دوره تمرینات پیلاتس بر شاخصهای منتخب کنترل حرکتی و عوامل مؤثر در آن در زنان سالمند غیرفعال انجام شد.
روش مطالعه
این تحقیق از نوع نیمهتجربی با طرح پیشآزمون و پسآزمون با گروه کنترل بود که روی 43 زن غیرفعال سالمند با دامنه سنی4/1±64/5 سال انجام شد که فعالیت بدنی کم، درد کمر نامعین، درصد چربی بدن بیش از ۳۵ درصد، نسبت دور کمر به لگن بیشتر از 0/95داشتند و برای دریافت برنامه ورزشی به مرکز مشاوره ورزشی و سلامت مراجعه کرده بودند. بدین ترتیب، نمونهها بهصورت تصادفی به دو گروه تجربی (22=n) و کنترل (21=n) تقسیم شدند. از افراد گروه تجربی 3 نفر از ادامه کار منصرف شدند.
قبل از شروع دوره تمرینی، برای اطلاع از وضعیت سلامتی و سطح آمادگی افراد، به ترتیب از پرسشنامه تاریخچه پزشکی و پرسشنامه آمادگی برای فعالیت جسمانی [9] استفاده شد که همه آزمودنیهای گروه تجربی شرایط احراز برای ورود به برنامه تمرینی را داشتند. پرسشنامه آمادگی برای فعالی جسمانی (PAR-Q) برگهای شامل هفت سؤال بلی و خیر است که برای گزینش افراد هنگام شرکت در فعالیتهای جسمانی که ممکن است برای آنها شدید باشد، طراحی شده است. PAR-Q بهعنوان استاندارد کمیته برای ورود به برنامههای تمرینی با شدت متوسط توصیه شده است. سؤالات طراحیشده در این پرسشنامه در حیطه سلامت قلب و عروقی، ناراحتیهای مفصلی و فشارخون افراد است [9]. گروه تجربی تمرینات پیلاتس را 3 جلسه در هر هفته به مدت چهار ماه انجام دادند؛ درحالیکه گروه کنترل به فعالیتهای روزمره خود مشغول بودند. دادهها با استفاده از آزمون آماری تی مستقل و تی وابسته در نرمافزار SPSS تحلیل شدند.
معیارهای ورود به مطالعه
تمایل به شرکت در تحقیق (امضای فرم رضایتنامه)، محدوده سنی 40 تا 50، دارای تجربه کمردرد نامعین در یک سال گذشته، درصد چربی بدن بیش از ۳۵ درصد، نسبت دور کمر به لگن ببیش 90 صدم، شرایط ورود به اجرای برنامه تمرینی با پرسشنامه تشخیصی PARQ، استفادهنکردن از داروهای اعصاب اثرگذار بر تعادل، نداشتن سابقهٔ آسیب اندام تحتانی در طول یک سال گذشته.
اندازهگیری میزان کمردرد
برای ارزیابی کمردرد از پرسشنامهای 9مادهای برای طبقهبندی درد افراد استفاده شد که هم عوامل فیزیکی و هم عوامل روانی درد را مشخص میکند. پایایی این آزمون 0/79گزارش شده است [10]. برای اندازهگیری میزان درد، از مقیاس بصری شدت درد برحسب درصد استفاده شد. این مقیاس نوار افقی به طول 100 میلیمتر یا 10 سانتیمتر است که یک انتهای آن صفر یعنی بدون درد و انتهای دیگر آن عدد 10 یعنی شدیدترین درد ممکن در نظر گرفته شده بود. از بیمار خواسته میشد تا ضمن نگاهکردن به پیوستار مذکور، میزان دردی را که در آن لحظه احساس میکرد، روی آن تعیین کند. پایایی داخلی این مقیاس بر اساس پژوهشهای قبلی 0/91=ICC گزارش شده است [11].


References
Full-Text: (5165 Views)
Extended Abstract
1. Introduction
Studies indicate the progressive degeneration of the nervous system and loss of physiological function in elderly people [1]. Since musculoskeletal disorders are one of the most common problems in the elderly, it is important to provide a strategy for its prevention or control. In this regard, low back pain is more common in people with inactive lifestyle [2], increased body mass index, especially in the abdominal region, and muscle weakness in central areas. With the increase in abdominal obesity, the compensatory curve is created in the lumbar curvature which increases pressure on the intervertebral discs [2]. Due to the increase in the curves of the lumbar region, the center of gravity moves forward and causes changes in how to walk, disturbance in postural control and increased risk of falling, and finally reduction in motor function [3], including a reduction
1. Introduction
Studies indicate the progressive degeneration of the nervous system and loss of physiological function in elderly people [1]. Since musculoskeletal disorders are one of the most common problems in the elderly, it is important to provide a strategy for its prevention or control. In this regard, low back pain is more common in people with inactive lifestyle [2], increased body mass index, especially in the abdominal region, and muscle weakness in central areas. With the increase in abdominal obesity, the compensatory curve is created in the lumbar curvature which increases pressure on the intervertebral discs [2]. Due to the increase in the curves of the lumbar region, the center of gravity moves forward and causes changes in how to walk, disturbance in postural control and increased risk of falling, and finally reduction in motor function [3], including a reduction
in walking speed and balance that results in reduced functional independence. In this regard, this study aimed to examine the effect of Pilates exercises on motor performance and low back pain in elderly women.
2. Methods and Materials
This study is a quasi-experimental study with control group using pretest and posttest conducted on 43 inactive elderly women with a mean (SD) age of 64.4 (5.1) year. The subjects were randomly divided into groups of test (n=22) and control (n=21). The Physical Activity Readiness Questionnaire (PAR-Q) was used to select samples to enter the study [2]. The test group performed Pilates exercises 3 sessions per week for 4 months. The inclusion criteria were as follows: 60 years or older, with non-specific low back pain in the past year, body fat percentage (BFP) higher than 35%, waist-hip ratio above 0.90, no problem for performing exercises, no medication use, and no history of lower limb injury during the past year. This study was approved by Ethics Committee of Imam Khomeini International University under code No. 17682. The Keele STarT Back Screening Tool (SBST) (9-item version) was used to measure low back pain which help physicians identify psychological and physical risk factors for pain [3]. The obesity variables (BFP and visceral fat) were measured by inBody 320 Body Composition Analyzer (InBody Co., Korea) [4]. To measure the speed of the subjects, 10-m sprint test, and to predict the risk of falling, Timed Up and Go test (TUG) were applied. Independent and dependent t test were performed to analyze the collected data.
3. Result
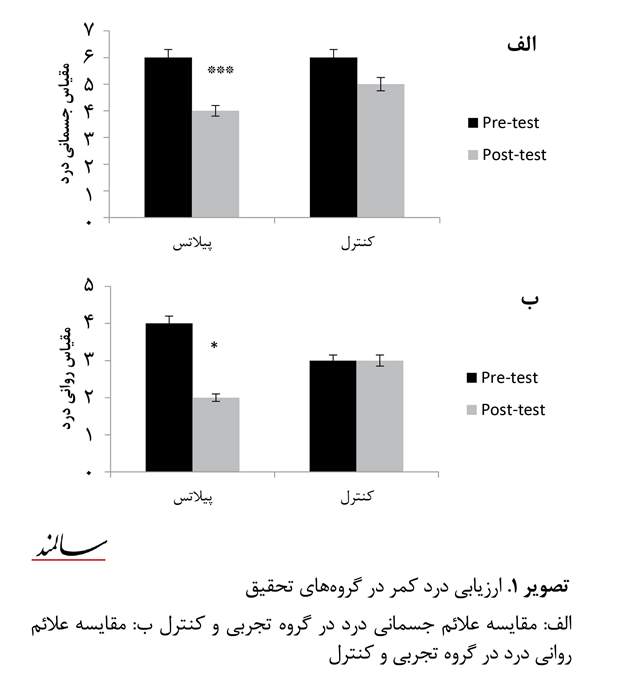
The results of this study showed that muscle volume (P=0.03) and abdominal obesity (P=0.001) in subjects with physical activity (test group) significantly improved compared to the control group. Physical (Figure 1a) and psychological symptoms of low back pain (Figure 1b) significantly improved after intervention with Pilates exercises (P=0.001).
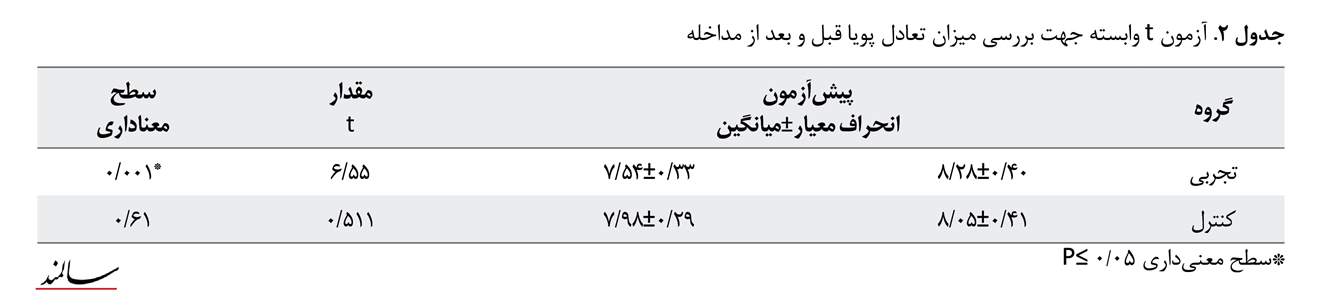
The results of dependent t test presented in Table 1, indicate that the dynamic balance of participants in test
2. Methods and Materials
This study is a quasi-experimental study with control group using pretest and posttest conducted on 43 inactive elderly women with a mean (SD) age of 64.4 (5.1) year. The subjects were randomly divided into groups of test (n=22) and control (n=21). The Physical Activity Readiness Questionnaire (PAR-Q) was used to select samples to enter the study [2]. The test group performed Pilates exercises 3 sessions per week for 4 months. The inclusion criteria were as follows: 60 years or older, with non-specific low back pain in the past year, body fat percentage (BFP) higher than 35%, waist-hip ratio above 0.90, no problem for performing exercises, no medication use, and no history of lower limb injury during the past year. This study was approved by Ethics Committee of Imam Khomeini International University under code No. 17682. The Keele STarT Back Screening Tool (SBST) (9-item version) was used to measure low back pain which help physicians identify psychological and physical risk factors for pain [3]. The obesity variables (BFP and visceral fat) were measured by inBody 320 Body Composition Analyzer (InBody Co., Korea) [4]. To measure the speed of the subjects, 10-m sprint test, and to predict the risk of falling, Timed Up and Go test (TUG) were applied. Independent and dependent t test were performed to analyze the collected data.
3. Result
The results of this study showed that muscle volume (P=0.03) and abdominal obesity (P=0.001) in subjects with physical activity (test group) significantly improved compared to the control group. Physical (Figure 1a) and psychological symptoms of low back pain (Figure 1b) significantly improved after intervention with Pilates exercises (P=0.001).
The results of dependent t test presented in Table 1, indicate that the dynamic balance of participants in test
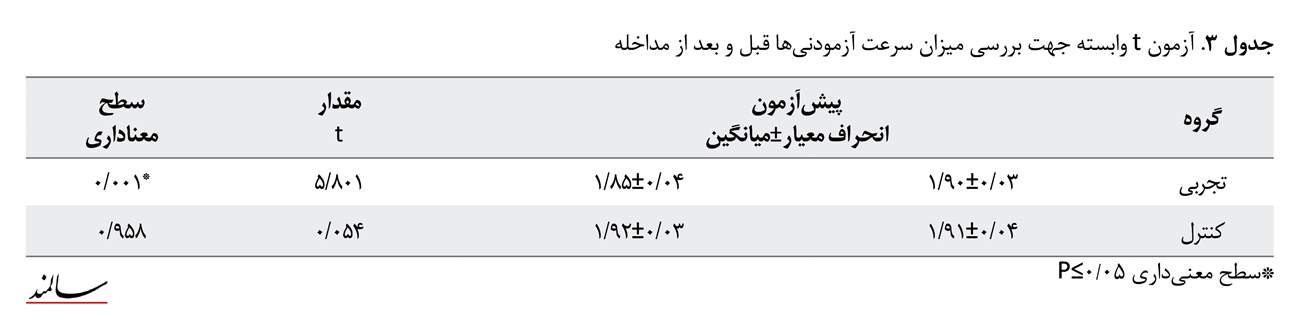
group significantly improved (P=0.001, t=6.55), while there was no significant difference in control group (t=0.51, P=0.616). According to the walking speed results in Table 2, there was a significant difference in the posttest results of test group (P=0.001, t=5.801), while no significant difference was found in control group (P=0.958, t=0.054).
4. Conclusion
The positive effects of Pilates exercises on the variables of body composition, back pain, and walking speed will improve the functional independence of the elderly. It was found out that Pilates exercises can reduce the physical and psychological symptoms of low back pain as well as abdominal and visceral obesity, and improve balance and walking speed. Since there was a direct relationship between abdominal obesity and low back pain; one of the possible causes of improving back pain in the Pilates group is the reduction in abdominal obesity. The mechanism of Pilates exercise training focuses on the development of comprehensive power where strength and endurance of the muscles increase; this improvement in the open-chain movement is effective in controlling the movement of the lower and upper limbs which results in improvement of functional factors [6]. Hence, Pilates exercises can improve the motor function of the elderly and cause a functional independency.
Ethical Considerations
Compliance with ethical guidelines
This study was referred to the Ethics and Research Council of Imam Khomeini International University for ethical review, and was performed after obtaining permission from the committee (No. 17682) was taken. Before the study began, the research process including the research objectives, how to measure variables, how to do the research program, and the length of the research period was explained to the participants. All participants volunteered to participate in the study, completing the consent.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere.
Acknowledgements
Hereby, we appreciate all the participants who helped us in conducting this research.
4. Conclusion
The positive effects of Pilates exercises on the variables of body composition, back pain, and walking speed will improve the functional independence of the elderly. It was found out that Pilates exercises can reduce the physical and psychological symptoms of low back pain as well as abdominal and visceral obesity, and improve balance and walking speed. Since there was a direct relationship between abdominal obesity and low back pain; one of the possible causes of improving back pain in the Pilates group is the reduction in abdominal obesity. The mechanism of Pilates exercise training focuses on the development of comprehensive power where strength and endurance of the muscles increase; this improvement in the open-chain movement is effective in controlling the movement of the lower and upper limbs which results in improvement of functional factors [6]. Hence, Pilates exercises can improve the motor function of the elderly and cause a functional independency.
Ethical Considerations
Compliance with ethical guidelines
This study was referred to the Ethics and Research Council of Imam Khomeini International University for ethical review, and was performed after obtaining permission from the committee (No. 17682) was taken. Before the study began, the research process including the research objectives, how to measure variables, how to do the research program, and the length of the research period was explained to the participants. All participants volunteered to participate in the study, completing the consent.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
All authors certify that this manuscript has neither been published in whole nor in part nor being considered for publication elsewhere.
Acknowledgements
Hereby, we appreciate all the participants who helped us in conducting this research.
مقدمه
امروزه به دلیل اقتضائاتی که در کشور وجود دارد، نسبت جمعیت افراد سالمند به جوان دچار فزونی شده است. با افزایش سن، با وجود ورزش و فعالیت جسمانی، بافتهای عضلانی تحلیل میروند و بافتهای چربی افزایش مییابند؛ از طرفی تغییرات ترکی بدن میتواند زمینه افت عملکرد جسمانی و کنترل حرکتی را ایجاد کند. کمردرد یا درد ستون فقرات نیز از شایعترین عوارض عضلانیاسکلتی است که در دوره سالمندی بیشتر در افرادی مشاهده میشود که سبک زندگی غیرفعالی دارند [1]. یکی از عواملی که ممکن است باعث درد کمر در دوره سالمندی شود، تغییرات ترکیب بدن اعمّ از افزایش توده چربی بدن به ویژه در ناحیه شکم و تحلیلرفتن عضلات در نواحی مرکزی بدن است.
با افزایش چاقی شکمی، قوسی جبرانی در ناحیه انحنای کمری ایجاد میشود. افزایش وزن بالاتنه نیز به دیسکهای بینمهرهای فشار زیادی میآورد و موجب کمردرد میشود [2]. در اثر افزایش قوس ناحیه کمری مرکز ثقل به سمت جلو جابهجا میشود و سبب تغییرات در نحوه گامبرداشتن، اختلال در کنترل پاسچر، افزایش خطر زمینخوردن و کاهش قابلیت جابهجایی حرکتی میشود [3].
یکی از روشهای ورزشی که در سالهای اخیر متخصصان ورزشی و توانبخشی به آن توجه کردهاند و در حال فراگیرشدن است، ورزش پیلاتس است. جوزف پیلاتس در سال 1880 این ورزش را برای اولینبار ابداع کرد. این ورزش مجموعهای از تمرینات تخصصی است که با هدف افزایش قدرت، استقامت و انعطافپذیری، بدن را تحت تأثیر قرار میدهد و از طرفی در کنار بهبود شرایط جسمانی به بهبود مسائل روانشناختی همچون توجه و تمرکز نیز کمک میکند [4]. کاهش بافت عضله در قسمت میانی بدن ممکن است موجب افزایش قوس کمری شود، این موضوع میتواند در سرعت راهرفتن افتی ایجاد کند. کاهش سرعت راهرفتن چنانچه به مقادیر کمتری از ۱ تا 2/1 متر بر ثانیه برسد، برای سالمندان مشکلاتی را در پی خواهد داشت [5]. با وجود تنوع زیاد شیوههای ورزشدرمانی، هنوز دلایل کافی درباره برتری یک روش بر دیگری وجود ندارد.
کائو و همکاران در سال ۲۰۰۷ طی تحقیقی عنوان کردند فعالیت و تمرینات بدنی منظم و مداوم میتواند بهطور مؤثری خطر افتادن را کاهش دهد و تحرک و ایمنی حرکت در زنان مسن را ارتقا بخشد [6]. همچنین آیرز در سال ۲۰۰۹ نشان داده است میتوان با انجام فعالیتهای جسمانی منظم در طول عمر، افت عملکرد حرکتی این افراد را تا حدودی به تأخیر انداخت [7]. سوزوکی و همکاران در سال ۲۰۰۹ طی تحقیقی نشان دادند تمرین و فعالیت بدنی باعث بهبود در تعادل، انعطافپذیری، قدرت عضلانی و توانایی راهرفتن، در افراد سالمند میشود [8].
با توجه به تحقیقات صورتگرفته، مشخص است درباره ورزش سالمندی تحقیقات متنوعی انجام شده است. این موضوع ضرورتی را ایجاد میکند تا در دوره قبلی سالمندی، تمهیداتی صورت پذیرد تا کیفیت زندگی در سالمندی به بهترین شکل تأمین شود. بنابراین، مطالعه حاضر با هدف تأثیر یک دوره تمرینات پیلاتس بر شاخصهای منتخب کنترل حرکتی و عوامل مؤثر در آن در زنان سالمند غیرفعال انجام شد.
روش مطالعه
این تحقیق از نوع نیمهتجربی با طرح پیشآزمون و پسآزمون با گروه کنترل بود که روی 43 زن غیرفعال سالمند با دامنه سنی4/1±64/5 سال انجام شد که فعالیت بدنی کم، درد کمر نامعین، درصد چربی بدن بیش از ۳۵ درصد، نسبت دور کمر به لگن بیشتر از 0/95داشتند و برای دریافت برنامه ورزشی به مرکز مشاوره ورزشی و سلامت مراجعه کرده بودند. بدین ترتیب، نمونهها بهصورت تصادفی به دو گروه تجربی (22=n) و کنترل (21=n) تقسیم شدند. از افراد گروه تجربی 3 نفر از ادامه کار منصرف شدند.
قبل از شروع دوره تمرینی، برای اطلاع از وضعیت سلامتی و سطح آمادگی افراد، به ترتیب از پرسشنامه تاریخچه پزشکی و پرسشنامه آمادگی برای فعالیت جسمانی [9] استفاده شد که همه آزمودنیهای گروه تجربی شرایط احراز برای ورود به برنامه تمرینی را داشتند. پرسشنامه آمادگی برای فعالی جسمانی (PAR-Q) برگهای شامل هفت سؤال بلی و خیر است که برای گزینش افراد هنگام شرکت در فعالیتهای جسمانی که ممکن است برای آنها شدید باشد، طراحی شده است. PAR-Q بهعنوان استاندارد کمیته برای ورود به برنامههای تمرینی با شدت متوسط توصیه شده است. سؤالات طراحیشده در این پرسشنامه در حیطه سلامت قلب و عروقی، ناراحتیهای مفصلی و فشارخون افراد است [9]. گروه تجربی تمرینات پیلاتس را 3 جلسه در هر هفته به مدت چهار ماه انجام دادند؛ درحالیکه گروه کنترل به فعالیتهای روزمره خود مشغول بودند. دادهها با استفاده از آزمون آماری تی مستقل و تی وابسته در نرمافزار SPSS تحلیل شدند.
معیارهای ورود به مطالعه
تمایل به شرکت در تحقیق (امضای فرم رضایتنامه)، محدوده سنی 40 تا 50، دارای تجربه کمردرد نامعین در یک سال گذشته، درصد چربی بدن بیش از ۳۵ درصد، نسبت دور کمر به لگن ببیش 90 صدم، شرایط ورود به اجرای برنامه تمرینی با پرسشنامه تشخیصی PARQ، استفادهنکردن از داروهای اعصاب اثرگذار بر تعادل، نداشتن سابقهٔ آسیب اندام تحتانی در طول یک سال گذشته.
اندازهگیری میزان کمردرد
برای ارزیابی کمردرد از پرسشنامهای 9مادهای برای طبقهبندی درد افراد استفاده شد که هم عوامل فیزیکی و هم عوامل روانی درد را مشخص میکند. پایایی این آزمون 0/79گزارش شده است [10]. برای اندازهگیری میزان درد، از مقیاس بصری شدت درد برحسب درصد استفاده شد. این مقیاس نوار افقی به طول 100 میلیمتر یا 10 سانتیمتر است که یک انتهای آن صفر یعنی بدون درد و انتهای دیگر آن عدد 10 یعنی شدیدترین درد ممکن در نظر گرفته شده بود. از بیمار خواسته میشد تا ضمن نگاهکردن به پیوستار مذکور، میزان دردی را که در آن لحظه احساس میکرد، روی آن تعیین کند. پایایی داخلی این مقیاس بر اساس پژوهشهای قبلی 0/91=ICC گزارش شده است [11].
اندازهگیری میزان فعالیت بدنی
بعد از توضیحات لازم و آشناکردن آزمودنیها، میزان فعالیت بدنی از طریق پرسشنامه فعالیت بدنی بک بهمنظور سنجش فعالیت بدنی آزمودنیها استفاده شد. این پرسشنامه مشتمل بر 16 سؤال در سه بخش فعالیت بدنی مربوط به اوقات فراغت، فعالیت ورزشی و فعالیت بدنی مربوط به شغل، تنظیم شده است. پایایی درونی پرسشنامه، با آزمون آلفای کرونباخ 0/79 گزارش شده است.
اندازهگیری ترکیب بدنی
متغیرهای چاقی شامل چاقی کلی بدن: شاخص درصد چربی بدن و چاقی احشایی: نسبت دور کمر به دور لگن، میزان چربی امعای احشایی با استفاده از دستگاه تحلیل ترکیب بدن (ساخت کشور کره جنوبی مدل (In Body 320) اندازهگیری شد.
اندازهگیری ۱۰متر سرعت راه رفتن
برای اندازهگیری سرعت آزمودنیها، از آنها خواسته شد که مسیری ۱۰متری را با حداکثر سرعت طی کنند. در این پژوهش، هر آزمودنی دومرتبه این آزمون را انجام داد که بهترین امتیاز او محاسبه شد. با تقسیم این عدد بر مسافت مدنظر، سرعت راهرفتن فرد برحسب متر بر ثانیه به دست آمد.
آزمون تعادل (زمان برخاستن و رفتن)
قبل از شروع تمرینات آزمون زمان برخاستن و رفتن (TUG) با پایایی ۹۹٪ برای پیشبینی خطر افتادن اجرا شد تا تعادل پویای شرکتکنندگان دو گروه کنترل و تجربی اندازهگیری شود [12]. آزمون به این صورت اجرا میشود که شرکتکننده بدون استفاده از دستهایش از روی صندلی بدون دسته برخاسته، پس از طیکردن مسیری سه متری بازمیگردد و دوباره روی صندلی مینشیند [13].
برنامه تمرینی
برای گروه تجربی که تحت تمرینات پیلاتس قرار گرفتند، در ابتدای هر جلسه تمرینی درباره چگونگی اجرای حرکات به آزمودنیها توضیحات اولیهای داده میشد. 10 دقیقه اول هر جلسه تمرینی به اجرای حرکات تنفسی پیلاتس اختصاص داشت، تمرینات اختصاصی در بازه زمانی 40 دقیقهای و درنهایت بازگشت به حالت اولیه و سردکردن به مدت پنج دقیقه اجرا شد. هفته اول تمرینی برای افزایش آمادگی عمومی بدن، هفته دوم و سوم با هدف افزایش قدرت (به کمک تمرینات با وزنه)، افزایش انعطاف (با چوب)، تمرینات کششی، هفته چهارم تا هشتم ترکیبی از تمرینات قدرتی، انعطافی و کششی انجام شد. در ماه سوم و چهارم این سیکل بهصورت ترکیبی از تمامی حرکات اجراشده در فازهای قبلی تکرار شد [4].
تحلیل دادهها
در مطالعه حاضر از آزمون آماری شاپیرو- ویلک برای ارزیابی عادیبودن دادهها و سپس از آزمون آماری تی مستقل و تی وابسته برای تحلیل آنها استفاده شد. در نهایت، دادهها در نرمافزار SPSS نسخه ۲۱ تحلیل شد. 05/0P≤ بهعنوان سطح معناداری در نظر گرفته شد.
یافتهها
نتایج آزمون t نشان داد حجم عضله آزمودنیهایی که فعالیت بدنی داشتند در مقایسه با گروه کنترل بهطور معنیداری افزایش یافته است (0/03=P). از طرف دیگر گروه تمرینی ورزش در آب، بهبود معنیداری در چاقی شکمی در دو متغیر نسبت دور کمر به دور لگن و چربی احشایی داشتند (0/001=P) (جدول شماره 1).
همانطور که در تصویر شماره 1 مشاهده میشود، الف) علائم جسمانی و ب) علائم روانی درد متعاقب اعمال برنامه
بعد از توضیحات لازم و آشناکردن آزمودنیها، میزان فعالیت بدنی از طریق پرسشنامه فعالیت بدنی بک بهمنظور سنجش فعالیت بدنی آزمودنیها استفاده شد. این پرسشنامه مشتمل بر 16 سؤال در سه بخش فعالیت بدنی مربوط به اوقات فراغت، فعالیت ورزشی و فعالیت بدنی مربوط به شغل، تنظیم شده است. پایایی درونی پرسشنامه، با آزمون آلفای کرونباخ 0/79 گزارش شده است.
اندازهگیری ترکیب بدنی
متغیرهای چاقی شامل چاقی کلی بدن: شاخص درصد چربی بدن و چاقی احشایی: نسبت دور کمر به دور لگن، میزان چربی امعای احشایی با استفاده از دستگاه تحلیل ترکیب بدن (ساخت کشور کره جنوبی مدل (In Body 320) اندازهگیری شد.
اندازهگیری ۱۰متر سرعت راه رفتن
برای اندازهگیری سرعت آزمودنیها، از آنها خواسته شد که مسیری ۱۰متری را با حداکثر سرعت طی کنند. در این پژوهش، هر آزمودنی دومرتبه این آزمون را انجام داد که بهترین امتیاز او محاسبه شد. با تقسیم این عدد بر مسافت مدنظر، سرعت راهرفتن فرد برحسب متر بر ثانیه به دست آمد.
آزمون تعادل (زمان برخاستن و رفتن)
قبل از شروع تمرینات آزمون زمان برخاستن و رفتن (TUG) با پایایی ۹۹٪ برای پیشبینی خطر افتادن اجرا شد تا تعادل پویای شرکتکنندگان دو گروه کنترل و تجربی اندازهگیری شود [12]. آزمون به این صورت اجرا میشود که شرکتکننده بدون استفاده از دستهایش از روی صندلی بدون دسته برخاسته، پس از طیکردن مسیری سه متری بازمیگردد و دوباره روی صندلی مینشیند [13].
برنامه تمرینی
برای گروه تجربی که تحت تمرینات پیلاتس قرار گرفتند، در ابتدای هر جلسه تمرینی درباره چگونگی اجرای حرکات به آزمودنیها توضیحات اولیهای داده میشد. 10 دقیقه اول هر جلسه تمرینی به اجرای حرکات تنفسی پیلاتس اختصاص داشت، تمرینات اختصاصی در بازه زمانی 40 دقیقهای و درنهایت بازگشت به حالت اولیه و سردکردن به مدت پنج دقیقه اجرا شد. هفته اول تمرینی برای افزایش آمادگی عمومی بدن، هفته دوم و سوم با هدف افزایش قدرت (به کمک تمرینات با وزنه)، افزایش انعطاف (با چوب)، تمرینات کششی، هفته چهارم تا هشتم ترکیبی از تمرینات قدرتی، انعطافی و کششی انجام شد. در ماه سوم و چهارم این سیکل بهصورت ترکیبی از تمامی حرکات اجراشده در فازهای قبلی تکرار شد [4].
تحلیل دادهها
در مطالعه حاضر از آزمون آماری شاپیرو- ویلک برای ارزیابی عادیبودن دادهها و سپس از آزمون آماری تی مستقل و تی وابسته برای تحلیل آنها استفاده شد. در نهایت، دادهها در نرمافزار SPSS نسخه ۲۱ تحلیل شد. 05/0P≤ بهعنوان سطح معناداری در نظر گرفته شد.
یافتهها
نتایج آزمون t نشان داد حجم عضله آزمودنیهایی که فعالیت بدنی داشتند در مقایسه با گروه کنترل بهطور معنیداری افزایش یافته است (0/03=P). از طرف دیگر گروه تمرینی ورزش در آب، بهبود معنیداری در چاقی شکمی در دو متغیر نسبت دور کمر به دور لگن و چربی احشایی داشتند (0/001=P) (جدول شماره 1).
همانطور که در تصویر شماره 1 مشاهده میشود، الف) علائم جسمانی و ب) علائم روانی درد متعاقب اعمال برنامه
تمرینی پیلاتس بهطور معناداری کاهشیافته است (0/001=P). همانطور که در تصویر شماره 2 مشاهده میشود، هر دو عامل چاقی شکمی (نسبت دور کمر به دور لگن و چربی احشایی) متعاقب اعمال برنامه تمرینی ورزش در آب بهطور معناداری کاهش یافت (0/001=P).
نتایج آزمون t وابسته در جدول شماره 2 آمده است. تعادل آزمودنیهای گروه تجربی (آزمون برخاستن و رفتن) در گروه تجربی بهبود معناداری داشت (T=-6/55 ، P=0/001)
، این در حالی بود که اختلاف معناداری در گروه کنترل مشاهده نشد (T=0/51 ، P=0/001). نتایج آزمون t مستقل نشان داد در پیشآزمون زمان برخاستن و رفتن بین گروه تجربی و کنترل، اختلاف معناداری وجود نداشت (0/51=P)، ولی در نمرات پسآزمون زمان برخاستن و رفتن بین گروه تجربی و کنترل اختلاف معناداری وجود داشت (0/001=P)،
، این در حالی بود که اختلاف معناداری در گروه کنترل مشاهده نشد (T=0/51 ، P=0/001). نتایج آزمون t مستقل نشان داد در پیشآزمون زمان برخاستن و رفتن بین گروه تجربی و کنترل، اختلاف معناداری وجود نداشت (0/51=P)، ولی در نمرات پسآزمون زمان برخاستن و رفتن بین گروه تجربی و کنترل اختلاف معناداری وجود داشت (0/001=P)،
همانطور که در جدول شماره 3 مشاهده میشود، نتایج آزمون t وابسته درونگروهی بین میانگین پیشآزمون و پسآزمون سرعت راه رفتن ۱۰متر در گروه تجربی اختلاف معناداری وجود دارد (T=-5/801 ، P=0/001)، درحالیکه این اختلاف برای گروه
کنترل معنیدار نبود(T=-0/054 ، P=0/958)، نتایج نشان داد در پیشآزمون سرعت راه رفتن ۱۰ متر بین گروه تجربی و کنترل، اختلاف معناداری وجود ندارد، ولی در نمرات پسآزمون زمان برخاستن و رفتن بین گروه تجربی و کنترل اختلاف معناداری وجود دارد.
بحث
هدف از مطالعه حاضر، بررسی تأثیر تمرینات پیلاتس بر متغیرهایی بود که میتوانند شاخصهای کنترل حرکتی را تحت تأثیر قرار دهند؛ عواملی مانند ترکیب بدن، درد کمر و سرعت راه رفتن که همگی قابلیت استقلال عملکردی را در زندگی اغنا میکنند. نتایج بهدستآمده نشان داد تمرینات پیلاتس باعث کاهش علائم جسمانی و روانی کمردرد نمونهها، کاهش چاقی شکمی WHR و چربی احشایی و همچنین بهبود تعادل و سرعت راه رفتن میشود.
چنانکه در مبانی نظری تحقیق عنوان شد ارتباط مستقیمی بین چاقی شکمی و درد کمر وجود دارد؛ بنابراین یکی از علل اصلی کاهش درد کمر در گروه پیلاتس را میتوان کاهش چاقی شکمی آنها دانست. آگاهی از اجزای بدن، استفاده هوشیارانه از عضلات، آگاهی از پیامهای عضلات و دامنه حرکتی مفاصل که از اصول اساسی تمرینات پیلاتس است، باعث جلوگیری از آسیبهای پرکاری، کشش و فشار بر عضلات میشود. اصل کشش در پیلاتس با تلفیق تمرکز بدن و حفظ راستای مناسب بدن کمک میکند تا عضلات در دامنه حرکتی کامل که برای
بحث
هدف از مطالعه حاضر، بررسی تأثیر تمرینات پیلاتس بر متغیرهایی بود که میتوانند شاخصهای کنترل حرکتی را تحت تأثیر قرار دهند؛ عواملی مانند ترکیب بدن، درد کمر و سرعت راه رفتن که همگی قابلیت استقلال عملکردی را در زندگی اغنا میکنند. نتایج بهدستآمده نشان داد تمرینات پیلاتس باعث کاهش علائم جسمانی و روانی کمردرد نمونهها، کاهش چاقی شکمی WHR و چربی احشایی و همچنین بهبود تعادل و سرعت راه رفتن میشود.
چنانکه در مبانی نظری تحقیق عنوان شد ارتباط مستقیمی بین چاقی شکمی و درد کمر وجود دارد؛ بنابراین یکی از علل اصلی کاهش درد کمر در گروه پیلاتس را میتوان کاهش چاقی شکمی آنها دانست. آگاهی از اجزای بدن، استفاده هوشیارانه از عضلات، آگاهی از پیامهای عضلات و دامنه حرکتی مفاصل که از اصول اساسی تمرینات پیلاتس است، باعث جلوگیری از آسیبهای پرکاری، کشش و فشار بر عضلات میشود. اصل کشش در پیلاتس با تلفیق تمرکز بدن و حفظ راستای مناسب بدن کمک میکند تا عضلات در دامنه حرکتی کامل که برای
تعادل عضلانی لازم است، کشیده شوند و همزمان عمل انقباض را انجام دهند، این کار با حمایت بدن انجام میشود [4]. از طرف دیگر کاهش چاقی شکمی که اساسی برای کاهش کمردرد است، در این تحقیق ذکر شد که همراستا با نتایج جیانپلو و همکاران و اسلنتز و همکاران است [15 ،14].
همچنین بهبود در وضعیت حفظ تعادل و سرعت راهرفتن با نتایج کائو و همکاران و ایواماتو و همکاران همسو بود [8 ،6]، اما با بخشی از نتایج آیرز و همکاران که عنوان کرد تمرینات استقامتی خشکی اثر معناداری بر سرعت راهرفتن ندارد، با این مطالعه مغایرت داشت [7]. اگرچه ماهیت برنامه تمرینی بهکاربردهشده در تحقیقات مشابه است، اما اختلافی که در نتایج بهدستآمده وجود دارد، میتواند ناشی از نادیدهگرفتن عواملی مانند میزان آمادگی آزمودنیها، سطح فعالیت بدنی، میزان انگیزش، جنسیت، سن، قد و وزن باشد. همچنین، تفاوت مشاهدهشده در تحقیقات را میتوان به دو روش تحقیق و متغیرهای دیگر نیز نسبت داد. با وجود اینکه قدرت عضلانی با افزایش سن کاهش مییابد [16]، در سالمندان قابل تعدیل است [17]. انجام تمرینات ورزشی، تغییرات عملکردی مرتبط با افزایش سن را جبران میکند و استقلال را در سنین سالمندی به مدت طولانیتری حفظ میکند. یافتههای مطالعات پیشنهاد میکند انجام فعالیت جسمانی منظم، ذخیره چربی بدن را کاهش میدهد و سبب افزایش قدرت و استقامت عضلانی و توانایی انجام فعالیتهای روزمره میشود.
آتروفی عضلانی نیز که با افزایش سن همراه است، از طریق انجام تمرینات قدرتی و پیلاتس میتواند به تأخیر افتد یا معکوس شود [16]. با توجه به اینکه ورزش پیلاتس در کشور ما ورزشی جدید به شمار میآید و از طرف دیگر، امکانات موردنیاز آن بسیار سهلالوصول است و در هر مکانی قابلیت اجرا دارد، توصیه میشود برای افزایش آمادگی عملکردی ازجمله سرعت، تعادل و ترکیب بدن و همچنین تقلیل دردهای جسمانی مرتبط با کمردرد داستفاده شود.
نتیجهگیری نهایی
با توجه به نتایج پژوهش حاضر، میتوان گفت که تمرینات پیلاتس به کاهش درصد چربی امعا و احشایی، درد کمر و بهبود در وضعیت تعادل و سرعت راهرفتن در سالمندان منجر میشود. ازاینرو، شرکت مستمر در فعالیتهای ورزشی پیلاتس قابلیت کاهش میزان چربی شکمی و بهبود کنترل عصبیعضلانی مرتبط با درد کمر و افزایش کیفیت حفظ تعادل و سرعت راه رفتن در سالمندان را دارد. این تمرینات با تقویت عضلات مرکزی بدن و تقویت عصبیعضلانی خط ثقل را در راستای طبیعی قرار میدهد و باعث ایجاد تعادل بدن در وضعیت مطلوبی میشود. درنتیجه ازاینگونه تمرینات در کنار دیگر برنامههای توانبخشی سالمندان میتوان استفاده کرد.
ملاحظات اخلاقی
پیروی از اصول اخلاق پژوهش
این مطالعه برای بررسی اخلاقی به شورای اخلاق و پژوهش دانشگاه بینالمللی امام خمینی (ره) ارجاع داده شد و پس از کسب مجوز از این کمیته به شماره ۱۷۶۸۲ انجام گرفت. قبل از شروع مطالعه، روند تحقیق شامل اهداف تحقیق، چگونگی اندازهگیری متغیرها، چگونگی انجام برنامه تمرینی و طول دوره تحقیق برای آزمودنیها توضیح داده شد. تمامی شرکتکنندگان داوطلبانه و با تکمیل رضایتنامه در تحقیق شرکت کردند.
حامی مالی
این مقاله حامی مالی ندارد.
تعارض منافع
بنا بر اظهار نظر نویسندگان این مقاله تعارض منافع ندارد.
تشکر و قدردانی
بدینوسیله از زحمات تمامی افرادی که در این مطالعه شرکت کردند و محقق را در اجرای این پژوهش یاری کردند، کمال تشکر و قدردانی میشود.
همچنین بهبود در وضعیت حفظ تعادل و سرعت راهرفتن با نتایج کائو و همکاران و ایواماتو و همکاران همسو بود [8 ،6]، اما با بخشی از نتایج آیرز و همکاران که عنوان کرد تمرینات استقامتی خشکی اثر معناداری بر سرعت راهرفتن ندارد، با این مطالعه مغایرت داشت [7]. اگرچه ماهیت برنامه تمرینی بهکاربردهشده در تحقیقات مشابه است، اما اختلافی که در نتایج بهدستآمده وجود دارد، میتواند ناشی از نادیدهگرفتن عواملی مانند میزان آمادگی آزمودنیها، سطح فعالیت بدنی، میزان انگیزش، جنسیت، سن، قد و وزن باشد. همچنین، تفاوت مشاهدهشده در تحقیقات را میتوان به دو روش تحقیق و متغیرهای دیگر نیز نسبت داد. با وجود اینکه قدرت عضلانی با افزایش سن کاهش مییابد [16]، در سالمندان قابل تعدیل است [17]. انجام تمرینات ورزشی، تغییرات عملکردی مرتبط با افزایش سن را جبران میکند و استقلال را در سنین سالمندی به مدت طولانیتری حفظ میکند. یافتههای مطالعات پیشنهاد میکند انجام فعالیت جسمانی منظم، ذخیره چربی بدن را کاهش میدهد و سبب افزایش قدرت و استقامت عضلانی و توانایی انجام فعالیتهای روزمره میشود.
آتروفی عضلانی نیز که با افزایش سن همراه است، از طریق انجام تمرینات قدرتی و پیلاتس میتواند به تأخیر افتد یا معکوس شود [16]. با توجه به اینکه ورزش پیلاتس در کشور ما ورزشی جدید به شمار میآید و از طرف دیگر، امکانات موردنیاز آن بسیار سهلالوصول است و در هر مکانی قابلیت اجرا دارد، توصیه میشود برای افزایش آمادگی عملکردی ازجمله سرعت، تعادل و ترکیب بدن و همچنین تقلیل دردهای جسمانی مرتبط با کمردرد داستفاده شود.
نتیجهگیری نهایی
با توجه به نتایج پژوهش حاضر، میتوان گفت که تمرینات پیلاتس به کاهش درصد چربی امعا و احشایی، درد کمر و بهبود در وضعیت تعادل و سرعت راهرفتن در سالمندان منجر میشود. ازاینرو، شرکت مستمر در فعالیتهای ورزشی پیلاتس قابلیت کاهش میزان چربی شکمی و بهبود کنترل عصبیعضلانی مرتبط با درد کمر و افزایش کیفیت حفظ تعادل و سرعت راه رفتن در سالمندان را دارد. این تمرینات با تقویت عضلات مرکزی بدن و تقویت عصبیعضلانی خط ثقل را در راستای طبیعی قرار میدهد و باعث ایجاد تعادل بدن در وضعیت مطلوبی میشود. درنتیجه ازاینگونه تمرینات در کنار دیگر برنامههای توانبخشی سالمندان میتوان استفاده کرد.
ملاحظات اخلاقی
پیروی از اصول اخلاق پژوهش
این مطالعه برای بررسی اخلاقی به شورای اخلاق و پژوهش دانشگاه بینالمللی امام خمینی (ره) ارجاع داده شد و پس از کسب مجوز از این کمیته به شماره ۱۷۶۸۲ انجام گرفت. قبل از شروع مطالعه، روند تحقیق شامل اهداف تحقیق، چگونگی اندازهگیری متغیرها، چگونگی انجام برنامه تمرینی و طول دوره تحقیق برای آزمودنیها توضیح داده شد. تمامی شرکتکنندگان داوطلبانه و با تکمیل رضایتنامه در تحقیق شرکت کردند.
حامی مالی
این مقاله حامی مالی ندارد.
تعارض منافع
بنا بر اظهار نظر نویسندگان این مقاله تعارض منافع ندارد.
تشکر و قدردانی
بدینوسیله از زحمات تمامی افرادی که در این مطالعه شرکت کردند و محقق را در اجرای این پژوهش یاری کردند، کمال تشکر و قدردانی میشود.
References
- Nachemson A, Waddell G, Norlund A. Epidemiology of neck and low back pain. In: Nachemson A, Jonsson E, editors. Neck and Back Pain: The Scientific Evidence of Causes, Diagnos is and Treatment. Philadelphia, Pennsylvania: Lippincott Williams & Wilkins; 2000.
- Ebenbichler GR, Oddsson LI, Kollmitzer J, Erim Z. Sensory-motor control of the lower back: Implications for rehabilitation. Medicine & Science in Sports & Exercise. 2001; 33(11):1889-98. [DOI:10.1097/00005768-200111000-00014]
- Wright VJ, Perricelli BC. Age-related rates of decline in performance among elite senior athletes. The American Journal of Sports Medicine. 2008; 36(3):443-50. [DOI:10.1177/0363546507309673] [PMID]
- Critchley DJ, Pierson Z, Battersby G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Manual Therapy. 2011; 16(2):183-9. [DOI:10.1016/j.math.2010.10.007] [PMID]
- Hoxie RE, Rubenstein LZ. Are older pedestrians allowed enough time to cross intersections safely? Journal of the American Geriatrics Society. 1994; 42(3):241-4. [DOI:10.1111/j.1532-5415.1994.tb01745.x]
- Cao ZB, Maeda A, Shima N, Kurata H, Nishizono H. The effect of a 12-week combined exercise intervention program on physical performance and gait kinematics in community-dwelling elderly women. Journal of Physiological Anthropology. 2007; 26(3):325-32. [DOI:10.2114/jpa2.26.325]
- Irez B. Pilates exercise positively affects balance, reaction time, muscle strength, number of falls and psychological parameters in 65+ years old women [PhD dissertation]. Ankara: Middle East Technical University; 2009.
- Iwamoto J, Suzuki H, Tanaka K, Kumakubo T, Hirabayashi H, Miyazaki Y, et al. Preventative effect of exercise against falls in the elderly: A randomized controlled trial. Osteoporosis International. 2009; 20(7):1233-40. [DOI:10.1007/s00198-008-0794-9] [PMID]
- Thomas S, Reading J, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Canadian Journal of Sport Sciences. 1992; 17(4):338-45. [PMID]
- Hill JC, Dunn KM, Main CJ, Hay EM. Subgrouping low back pain: a comparison of the STarT Back Tool with the Örebro Musculoskeletal Pain Screening Questionnaire. European Journal of Pain. 2010; 14(1):83-9. [DOI:10.1016/j.ejpain.2009.01.003] [PMID] [PMCID]
- Karimi A. A prospective study of the outcome of treatment of chronic low back pain patients with consistent and inconsistent clinical signs as defined by three screening tests [MSc. thesis]. Norwich: University of East Anglia; 2004.
- Lopopolo RB, Greco M, Sullivan D, Craik RL, Mangione KK. Effect of therapeutic exercise on gait speed in community-dwelling elderly people: A meta-analysis. Physical Therapy. 2006; 86(4):520-40. [PMID]
- Buchner DM, Cress ME, De Lateur BJ, Esselman PC, Margherita AJ, Price R, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 1997; 52(4):M218-M24. [DOI:10.1093/gerona/52A.4.M218] [PMID]
- Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, Samsa GP, et al. Effects of the amount of exercise on body weight, body composition, and measures of central obesity: STRRIDE—a randomized controlled study. Archives of internal medicine. 2004; 164(1):31-9. [DOI:10.1001/archinte.164.1.31] [PMID]
- Giannopoulou I, Ploutz-Snyder L, Carhart R, Weinstock R, Fernhall B, Goulopoulou S, et al. Exercise is required for visceral fat loss in postmenopausal women with type 2 diabetes. The Journal of Clinical Endocrinology & Metabolism. 2005; 90(3):1511-8. [DOI:10.1210/jc.2004-1782] [PMID]
- Md JFB, Kiely DK, Herman S, Leveille SG, Mizer K, Frontera WR, et al. The relationship between leg power and physical performance in mobility-limited older people. Journal of the American Geriatrics Society. 2002; 50(3):461-7. [DOI:10.1046/j.1532-5415.2002.50111.x]
- Rogers ME, Rogers NL, Takeshima N, Islam MM. Methods to assess and improve the physical parameters associated with fall risk in older adults. Preventive Medicine. 2003; 36(3):255-64. [DOI:10.1016/S0091-7435(02)00028-2]
Type of Study: Research |
Subject:
Rehabilitation Management
Received: 2018/03/03 | Accepted: 2018/07/19 | Published: 2018/10/01
Received: 2018/03/03 | Accepted: 2018/07/19 | Published: 2018/10/01
References
1. Nachemson A, Waddell G, Norlund A. Epidemiology of neck and low back pain. In: Nachemson A, Jonsson E, editors. Neck and Back Pain: The Scientific Evidence of Causes, Diagnos is and Treatment. Philadelphia, Pennsylvania: Lippincott Williams & Wilkins; 2000.
2. Ebenbichler GR, Oddsson LI, Kollmitzer J, Erim Z. Sensory-motor control of the lower back: Implications for rehabilitation. Medicine & Science in Sports & Exercise. 2001; 33(11):1889-98. [DOI:10.1097/00005768-200111000-00014] [DOI:10.1097/00005768-200111000-00014]
3. Wright VJ, Perricelli BC. Age-related rates of decline in performance among elite senior athletes. The American Journal of Sports Medicine. 2008; 36(3):443-50. [DOI:10.1177/0363546507309673] [PMID] [DOI:10.1177/0363546507309673]
4. Critchley DJ, Pierson Z, Battersby G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Manual Therapy. 2011; 16(2):183-9. [DOI:10.1016/j.math.2010.10.007] [PMID] [DOI:10.1016/j.math.2010.10.007]
5. Hoxie RE, Rubenstein LZ. Are older pedestrians allowed enough time to cross intersections safely? Journal of the American Geriatrics Society. 1994; 42(3):241-4. [DOI:10.1111/j.1532-5415.1994.tb01745.x] [DOI:10.1111/j.1532-5415.1994.tb01745.x]
6. Cao ZB, Maeda A, Shima N, Kurata H, Nishizono H. The effect of a 12-week combined exercise intervention program on physical performance and gait kinematics in community-dwelling elderly women. Journal of Physiological Anthropology. 2007; 26(3):325-32. [DOI:10.2114/jpa2.26.325] [DOI:10.2114/jpa2.26.325]
7. Irez B. Pilates exercise positively affects balance, reaction time, muscle strength, number of falls and psychological parameters in 65+ years old women [PhD dissertation]. Ankara: Middle East Technical University; 2009.
8. Iwamoto J, Suzuki H, Tanaka K, Kumakubo T, Hirabayashi H, Miyazaki Y, et al. Preventative effect of exercise against falls in the elderly: A randomized controlled trial. Osteoporosis International. 2009; 20(7):1233-40. [DOI:10.1007/s00198-008-0794-9] [PMID] [DOI:10.1007/s00198-008-0794-9]
9. Thomas S, Reading J, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Canadian Journal of Sport Sciences. 1992; 17(4):338-45. [PMID] [PMID]
10. Hill JC, Dunn KM, Main CJ, Hay EM. Subgrouping low back pain: a comparison of the STarT Back Tool with the Örebro Musculoskeletal Pain Screening Questionnaire. European Journal of Pain. 2010; 14(1):83-9. [DOI:10.1016/j.ejpain.2009.01.003] [PMID] [PMCID] [DOI:10.1016/j.ejpain.2009.01.003]
11. Karimi A. A prospective study of the outcome of treatment of chronic low back pain patients with consistent and inconsistent clinical signs as defined by three screening tests [MSc. thesis]. Norwich: University of East Anglia; 2004.
12. Lopopolo RB, Greco M, Sullivan D, Craik RL, Mangione KK. Effect of therapeutic exercise on gait speed in community-dwelling elderly people: A meta-analysis. Physical Therapy. 2006; 86(4):520-40. [PMID] [PMID]
13. Buchner DM, Cress ME, De Lateur BJ, Esselman PC, Margherita AJ, Price R, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 1997; 52(4):M218-M24. [DOI:10.1093/gerona/52A.4.M218] [PMID] [DOI:10.1093/gerona/52A.4.M218]
14. Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, Samsa GP, et al. Effects of the amount of exercise on body weight, body composition, and measures of central obesity: STRRIDE—a randomized controlled study. Archives of internal medicine. 2004; 164(1):31-9. [DOI:10.1001/archinte.164.1.31] [PMID] [DOI:10.1001/archinte.164.1.31]
15. Giannopoulou I, Ploutz-Snyder L, Carhart R, Weinstock R, Fernhall B, Goulopoulou S, et al. Exercise is required for visceral fat loss in postmenopausal women with type 2 diabetes. The Journal of Clinical Endocrinology & Metabolism. 2005; 90(3):1511-8. [DOI:10.1210/jc.2004-1782] [PMID] [DOI:10.1210/jc.2004-1782]
16. Md JFB, Kiely DK, Herman S, Leveille SG, Mizer K, Frontera WR, et al. The relationship between leg power and physical performance in mobility-limited older people. Journal of the American Geriatrics Society. 2002; 50(3):461-7. [DOI:10.1046/j.1532-5415.2002.50111.x] [DOI:10.1046/j.1532-5415.2002.50111.x]
17. Rogers ME, Rogers NL, Takeshima N, Islam MM. Methods to assess and improve the physical parameters associated with fall risk in older adults. Preventive Medicine. 2003; 36(3):255-64. [DOI:10.1016/S0091-7435(02)00028-2] [DOI:10.1016/S0091-7435(02)00028-2]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
